
The diagnostic silence that follows a “clear” angiogram in a symptomatic heart attack patient is perhaps one of the most unsettling experiences in modern clinical practice. While traditional X-ray imaging has served as the gold standard for decades, it often fails to detect the subtle, microscopic pathologies that occur within the vessel walls or the heart muscle itself. This gap is most evident in cases of Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA), where the absence of a visible blockage frequently leads to misdiagnosis or therapeutic stagnation. Multimodal cardiac imaging has emerged as a disruptive framework, synthesizing different physical principles to visualize what was previously invisible, thereby transforming the “unexplained” heart attack into a treatable condition.
This technological evolution represents a shift from macro-level observation toward cellular-level interrogation. Instead of relying on a single modality that might only capture 50% of the clinical picture, modern frameworks integrate structural, functional, and molecular data. The relevance of this synergy cannot be overstated; in a landscape where personalized medicine is the objective, the ability to differentiate between a subtle plaque rupture and heart muscle inflammation determines whether a patient receives aggressive anti-clotting medication or anti-inflammatory therapy. By combining diverse imaging streams, clinicians can finally bypass the limitations of traditional luminology—the study of the “hole” in the vessel—to examine the actual biological landscape of the heart.
Introduction to Multimodal Diagnostic Frameworks
The emergence of multimodal diagnostic frameworks is a direct response to the complexity of cardiovascular disease, which rarely manifests through a single pathway. At its core, this technology involves the synchronized use of different imaging sensors to create a composite map of the cardiovascular system. It functions by layering the high-resolution architectural data of the coronary arteries over the deep-tissue metabolic and structural information of the myocardium. This context is vital because it moves away from a “one-size-fits-all” diagnostic approach, acknowledging that a heart attack can be a plumbing issue, an electrical failure, or an inflammatory response.
In the broader technological landscape, these frameworks represent the pinnacle of data fusion in healthcare. By integrating different physical signals—light waves for internal vessel mapping and radiofrequency pulses for muscle characterization—the system eliminates the blind spots inherent in any single-modality approach. This implementation is unique because it does not just provide more images; it provides a hierarchical diagnostic path. It allows for a “search and rescue” mission within the human body, where one tool identifies the general area of distress and the second identifies the exact cause of the emergency.
Core Imaging Components and Technical Synergy
Optical Coherence Tomography (OCT)
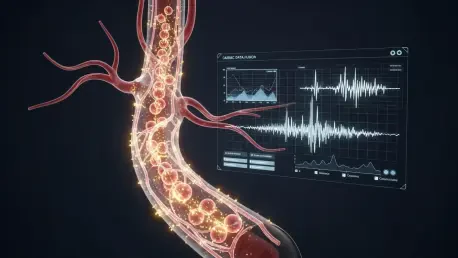
Optical Coherence Tomography (OCT) functions as the “microscope from within,” using near-infrared light to provide cross-sectional views of the coronary artery with a resolution of approximately 10 to 20 microns. This performance is nearly ten times sharper than traditional intravascular ultrasound, allowing clinicians to see the ultra-thin fibrous caps of plaques that are prone to rupture. The significance of OCT in the overall system lies in its ability to detect “soft” triggers—such as erosion or small blood clots—that do not result in a total blockage but are enough to cause significant cardiac damage.
Beyond mere visualization, OCT provides a structural assessment that changes the surgical or medicinal trajectory for the patient. For example, by identifying a spontaneous coronary artery dissection—a tear in the vessel wall—OCT prevents the unnecessary and potentially dangerous placement of a stent. It acts as the primary investigative tool for the “pipes,” ensuring that any vascular injury, no matter how microscopic, is documented. This level of detail is the first critical pillar in the multimodal framework, narrowing down the search for a cause to the vascular level before the focus shifts to the muscle itself.
Cardiac Magnetic Resonance Imaging (MRI)
While OCT investigates the internal channels, Cardiac Magnetic Resonance Imaging (MRI) offers an in-depth look at the heart’s “engine room.” By utilizing powerful magnetic fields and radio waves, it identifies the specific signature of tissue damage, such as edema or scarring. Its performance characteristics are unique because it can distinguish between ischemic damage (caused by lack of blood flow) and non-ischemic damage (caused by infection or stress). This distinction is vital; a patient whose MRI shows myocarditis requires an entirely different recovery protocol than one whose MRI shows a classic, albeit small, infarction.
The real-world usage of cardiac MRI within a multimodal framework provides the final piece of the diagnostic puzzle. It can reveal “mimic” conditions like Takotsubo syndrome, where the heart temporarily deforms due to extreme stress, appearing like a heart attack on initial tests. By analyzing the patterns of gadolinium enhancement within the muscle, the MRI serves as a functional validator of the OCT findings. If the OCT shows a clear vessel but the MRI shows localized muscle death, it forces the clinician to look for transient causes, such as a temporary spasm that has already resolved but left a permanent mark.
Current Trends and Investigative Paradigms
The current trajectory of cardiac imaging is defined by a shift toward prospective, data-driven protocols that prioritize immediate, comprehensive testing over traditional “watchful waiting.” One of the most significant innovations is the move toward simultaneous or “near-simultaneous” imaging, where patients move directly from the catheterization lab to the MRI suite. This trend is heavily influenced by the realization that cardiac biomarkers alone are insufficient; even patients with mild symptoms often harbor significant tissue damage that only specialized imaging can reveal.
Moreover, there is an emerging industry shift toward inclusive diagnostic modeling. Recent investigative paradigms have debunked the myth that men and women require different biological explanations for heart attacks; rather, they require more precise tools to see the same underlying mechanisms. The focus is now on creating standardized “imaging bundles” that ensure every patient, regardless of demographic, receives the same high-level interrogation of their cardiac health. This shift is turning the diagnostic process from an expert’s intuition into a rigorous, tech-enabled evidence gathering exercise.
Clinical Applications in Coronary Assessment
The most notable implementation of this technology is found in specialized heart attack research programs across global academic medical centers. In these environments, the dual-imaging protocol is deployed as a frontline defense for patients who present with atypical heart attack profiles. For instance, in the sector of emergency cardiology, this framework is used to prevent the premature discharge of patients who have “normal” angiograms but are actually suffering from microscopic vessel ruptures. These real-world applications have turned the diagnostic success rate from a coin flip into a near-certainty.
A unique use case involves the management of young, otherwise healthy patients who experience sudden cardiac events. In these scenarios, the technology is used to identify rare vascular conditions or silent inflammatory triggers that standard tests miss. By deploying OCT and MRI in tandem, these centers can provide a definitive “why” to the patient, which is often as important for long-term psychological recovery as the physical treatment itself. This implementation has effectively bridged the gap between the emergency room and the long-term preventive clinic.
Implementation Hurdles and Technical Limitations
Despite its diagnostic prowess, the technology faces substantial hurdles, primarily concerning the logistical friction of coordinating two high-complexity tests. The technical challenge lies in the “time-is-muscle” reality of cardiology; while OCT is performed during the initial catheterization, an MRI requires transporting a potentially unstable patient to a different wing of the hospital. This geographical and procedural separation can delay definitive diagnosis, which is why ongoing development efforts are focusing on integrated imaging suites where both modalities can be accessed more seamlessly.
Regulatory and economic obstacles also affect widespread adoption. These advanced imaging tools are expensive and require highly specialized technicians to interpret the data accurately. In many regional hospitals, the lack of 24/7 access to cardiac MRI means that the “multimodal” promise remains unfulfilled for a large portion of the population. Furthermore, the invasive nature of OCT, which requires inserting a catheter into the heart, carries its own set of minor risks, making some clinicians hesitant to use it if they believe a non-invasive MRI might suffice—even though the data shows both are often necessary for a complete picture.
Future Outlook and Precision Medicine
The future of this technology is headed toward a fusion of imaging and artificial intelligence to provide real-time, predictive analytics. We are moving toward a period where machine learning algorithms will assist in the interpretation of OCT scans, highlighting microscopic tears that might be missed by the human eye during a high-stress procedure. This will likely lead to “precision cardiology,” where a patient’s specific imaging “fingerprint” dictates their exact medication dosage, moving away from generalized prescriptions toward a truly individualized recovery plan.
In the long term, the impact of these advancements will likely redefine the standard of care for all cardiovascular events, not just MINOCA. As the technology becomes more miniaturized and the software more intuitive, we may see the integration of these high-res sensors into standard diagnostic tools. This will effectively eliminate the “mystery” from cardiology, ensuring that every patient leaves the hospital with a clear understanding of their cardiac architecture. The ultimate breakthrough will be the move from treating the damage to predicting it, using these high-resolution frameworks to identify vulnerable patients before an event even occurs.
Assessment of Diagnostic Efficacy
The shift toward multimodal cardiac imaging has effectively dismantled the era of diagnostic uncertainty for complex heart events. By combining the internal resolution of OCT with the tissue characterization of MRI, the medical community successfully identified definitive causes in nearly 80% of cases that were previously deemed mysteries. This framework moved beyond the limitations of traditional X-rays, proving that “normal” arteries often hide microscopic pathologies that require specific, targeted interventions. The technology demonstrated that high-resolution data fusion is not just a luxury, but a necessity for ensuring patient safety and therapeutic accuracy.
The implementation of these dual-imaging strategies provided a clear roadmap for the future of precision medicine. It highlighted the fact that symptoms and blood tests alone could not reliably predict the underlying cause of a heart attack, necessitating a specialized technological approach for every patient. While logistical and cost-related hurdles remained, the evidence for improved clinical outcomes was undeniable. This paradigm shift ensured that patients, especially women and younger individuals, were no longer dismissed due to clear angiograms. Ultimately, the adoption of these tools transformed cardiology from a reactive practice into a data-driven science, setting a new standard for diagnostic excellence.